Disaggregation of Wellbeing Indicators
 Go Back
Go Back 4.1: DATA AND METHODS
This study uses data from MICS6 for 35 countries. The MICS program is a household survey program supported by the United Nations Children’s Fund (UNICEF). Its main objective is to monitor the situation of children and women. MICS operates in multiyear rounds, generally adding new tools with each round. The program is currently in the sixth and largest round of surveys, with many surveys in Europe and Central Asia and West and Central Africa (Khan and Hancioglu 2019). MICS is designed to provide estimates for a large number of indicators for children and women at national and regional levels, for urban and rural areas. Interviews are conducted using tablet computers.
MICS6 uses several questionnaires: household, women aged 15–49 years, men aged 15–49 years (in selected countries only), children under age 5, children 5–17 years, and water-quality testing. For many countries, round 6 added the WGSS in an Adult Functioning module for women aged 18-49 and the Child Functioning Module for children age 2 to17 . The women questionnaire is administered to all women in a household aged 15 to 49. In some countries, the MICS6 men’s questionnaire was administered to eligible households. The households were randomly selected and one aged 15 to 49 was randomly selected to complete the questionnaire.
We selected MICS6 datasets available for public use as of December 2021 and that includes the WGSS in the women’s questionnaire. We use MICS6 datasets collected from 2017 to 2020 in the following 35 countries: Algeria, Bangladesh, Belarus, Central African Republic, Chad, Costa Rica, Cuba, Dominican Republic, Democratic Republic of Congo, Georgia, Ghana, Guinea Bissau, Gambia, Guyana, Honduras, Iraq, Kiribati, Kosovo, Kyrgyz, Lesotho, Madagascar, Malawi, Mongolia, Montenegro, Nepal, North Macedonia, Palestine, Sao Tome, Sierra Leone, Suriname, Togo, Tonga, Tunisia, Turkmenistan, Zimbabwe.
A. DISABILITY MEASUREMENT
In the MICS6 datasets used in this Report, the WG-SS is included in the women questionnaire and not in the roster. Only women who are not considered to be ‘incapacitated’ by the survey staff at the start of the women’s questionnaire were administered the questionnaire. Women with functional difficulties that might interfere with answering the questionnaire were not given the opportunity to have a proxy respondent and did not answer the questionnaire.5
Women 50 years old and older do not answer functional difficulty questions, nor do adult men in most countries.[6] Hence, MICS cannot
be used to assess prevalence among adults. This study, therefore, does not present prevalence estimates among individuals and households. Instead, it focuses on assessing inequalities between women with and without functional difficulties.
It should be noted that the WG-SS has been slightly modified by first asking two questions on whether the person uses glasses and hearing aids. In this setting, seeing difficulties are captured as follows: we consider a person to have seeing difficulties whether they use glasses or not but report having difficulty seeing. Similarly, we consider a person to have difficulty hearing whether they use a hearing aid or not, but report having difficulty hearing.
Disability is only measured based on six functional difficulties. Therefore, it does not capture all persons with disabilities, particularly persons with psychosocial and mental health disabilities. Given the incomplete nature of the measure used in this study, we refer to ‘persons with functional difficulties’ and not persons with disabilities that constitute a wider group.
To identify a specific ‘functional difficulty status’ group, a threshold among functional difficulties needs to be defined. Recognizing that identification and categorization could lead to varying results depending on the threshold, the Results tables available on the disability data initiative website include results for the three categorizations below for women age 18 to 49 (Appendix 3 Method brief #1).
A. First, individuals are in two categories:
– ‘No difficulty’ for all domains.
– Any difficulty in at least one domain (respondents report at ‘Some difficulty’, or ‘A lot of difficulty’ or ‘Unable to do’ in at least one domain).
B. Second, individuals are in three categories:
– ‘No difficulty’ for all domains.
-‘Some difficulty’ in at least one domain but no ‘A lot of difficulty’ or ‘Unable to do’ responses across all domains.
– At least a lot of difficulty: ‘A lot of difficulty’ or ‘Unable to do’ in at least one domain.
C. Finally, following the recommendation of the Washington Group, individuals are grouped as follows:
– ‘No difficulty’ or ‘Some difficulty’ for all domains
– At least a lot of difficulty: ‘A lot of difficulty’ or ‘Unable to do’ in at least one domain.
The analysis below highlights more often categorization B above as it provides the most information and allows us to continue to explore if there is a gradient in the severity of functional difficulties and deprivations.
At the same time, to disaggregate indicators by functional domain (e.g., seeing), we focus on persons with any difficulty (categorization A) and do not separate persons with some or at least a lot of difficulty, given small sample sizes (below 50) for many countries for persons with at least a lot of difficulty.
B. INDICATORS
This Report uses indicators to capture the situation of persons with disabilities in various dimensions of wellbeing. The indicators are in Table 2.1 and described in Appendix 3 Method Brief #1. The list of indicators was developed by reviewing the MICS6 questionnaire and MICS indicators (UNICEF 2021a) considering the provisions of the CRPD and the SDGs that they inform (OHCHR 2021b).
This report and Results Data Tables on the DDI website compare indicators across groups by functional difficulty status to establish the size of the gap that may be associated with disability, i.e., the disability gap or inequality associated with disability. For each dataset and indicator, we set 50 observations as the minimum requirement to produce estimates disaggregated across functional difficulty status.
This minimum sample size of 50 has constrained the indicators that could be covered in this Report. Indeed, we did not include indicators that had missing data and brought the number of observations below 50 for many countries. For instance, this is the case for the share of women who were first married or in union before age 18. In addition, several MICS6 indicators (UNICEF 2021a) are based on subsamples of women, such as women with a live birth in the last two years. In many countries, such subsamples did not generate the 50 or more observations for women with functional difficulties.
Results are presented in tables at country and cross-country levels. Data analysis takes into account the complex survey design of MICS6. In the Results Tables, the difference across functional difficulty status and its statistical significance is noted in a separate column. Statistical significance is based on a t-test (*, **, and *** at the 10%, 5% and 1% levels respectively).
We use the term disability gap to refer to a difference that is statistically significant and refers to a disadvantage for persons with functional difficulties. There may be patterns of disadvantage that affect subgroups of persons with disabilities and their households, such as rural residents. Disability disaggregation of subgroups of the population by rural/urban and by age groups are reported in the DDI website for sample size greater than 50 observations.
Cross-country estimates are weighted averages of country estimates using population statistics for women ages 18 to 49 for 34 countries under study[7] (United Nations 2019a). Cross-country estimates do not represent the situation of all women globally. Instead, they reflect overall the situation of women in 34 countries.
C. DESCRIPTIVE STATISTICS
The countries and territories under study are described in Appendix 2.1 and represented in Figure 4.1. They are heterogenous in terms of life expectancy at birth, Gross National Income (GNI) per capita and human development index (HDI). For instance, life expectancy ranges from a low of 53 in Central African Republic to a high of 80 in Costa Rica. All but four countries have ratified the CRPD (OHCHR 2022).
Figure 4.1: Countries covered in this study
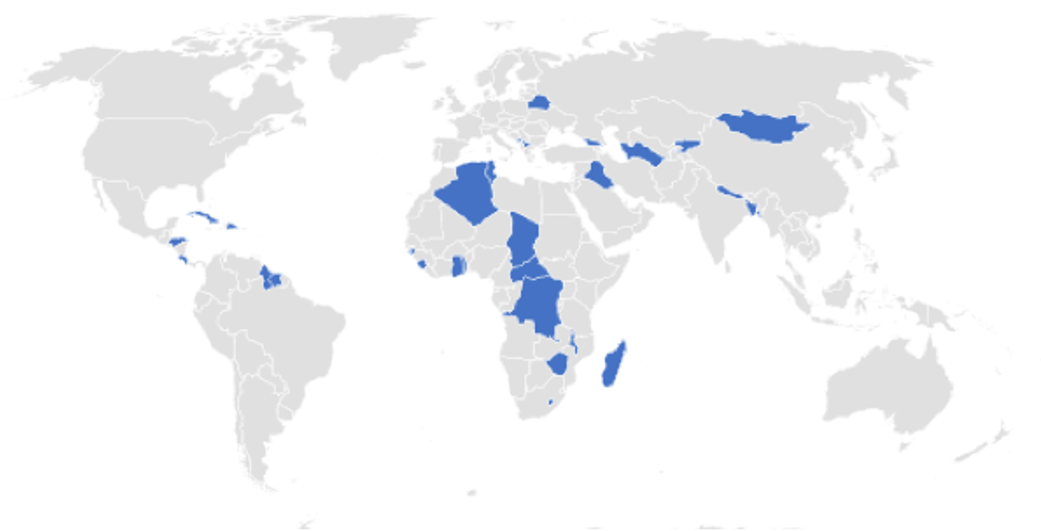
Descriptive statistics are in Appendix 2.2 for the sample of 418,527 women in 35 countries: the mean age of women in the sample ranges from 30 to 36. The share of women in rural areas varies from 21% in Belarus to 82% in Malawi.
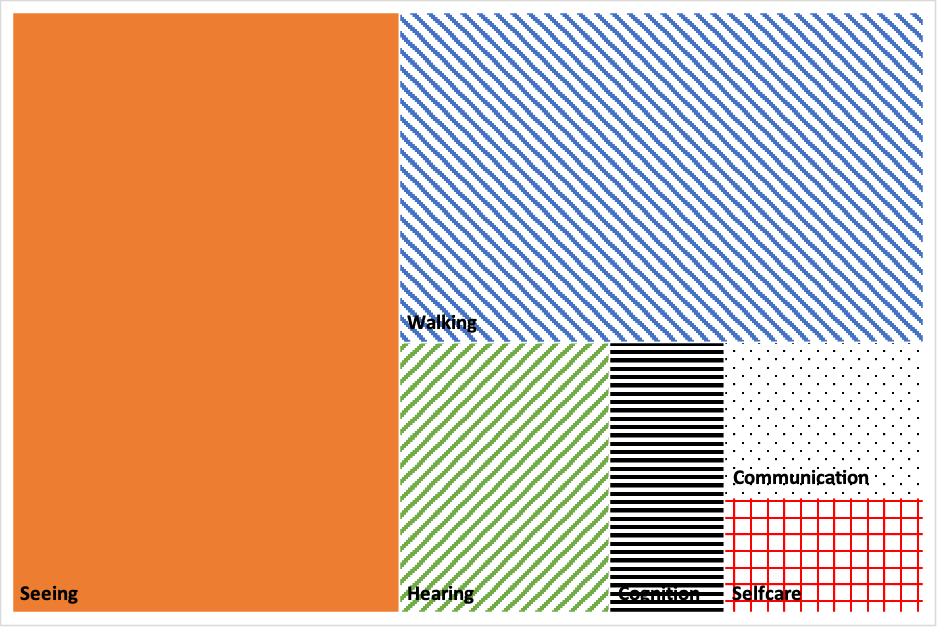
Among women with any functional difficulties, the share with a difficulty in each domain is shown in Appendix 2.4 for each country and in Figure 4.2 for all countries. The most common difficulties are seeing (51%), cognition (47%), walking (38%) followed by hearing (12%), communication (7%) and selfcare (5%). The total adds up to more than 100% as some women have difficulties in multiple domains.
Among women with seeing and hearing difficulties respectively, glasses and hearing aid use is presented in Appendix 2.5. As per cross-country estimates, 19% of women with seeing difficulties use glasses and 2% of women with hearing difficulties use hearing aids. This is consistent with recent results from WHO- UNICEF (2022) on unmet needs for assistive products worldwide.
D. LIMITATIONS
This analysis has limitations. First, we acknowledge the limitation of MICS data in identifying the functional difficulty status at the household level as only women ages 18 to 49 were administered the adult functioning questionnaire. Children were administered the child functioning module in the MICS6 under study, but we do not consider the functional status of children in this Report. In addition, our data does not capture the functional status of men of all ages[8] and women 50 and older and thus is not adequate to capture the functional status of adults in a household. It does not identify persons with a variety of disabilities, including psychosocial, neurological, and mental health ones, which are counted under persons with no difficulty.
Of course, the data does not include individuals who are not in a household, such as those who are homeless or institutionalized who may be at a disproportionate risk of functional difficulties and deprivations.
The data utilized does not adjust for mortality and may be affected by a mortality bias, as adults with functional difficulties may be disproportionately affected by premature mortality (Mitra 2018).
Second, although data comes from a single international survey program, results may not be perfectly comparable across countries. What persons may understand from the questionnaire across countries on various topics, on adult functioning in particular, and how they reply can differ given different languages, cultures, interviewer training, and other contextual factors in ways that are beyond the purview of the researchers.
The analyses presented in succeeding sections consider only two factors that may contribute to intersectional disadvantages for women with disabilities (area of residence (rural vs urban) and age group (age 18 to 29 and age 30 to 44), while others are not covered (e.g. immigration status, ethnicity, indigeneity, gender identity or sexual orientation). Finally, this Report provides descriptive statistics and bivariate analysis. It is silent on the causal effects of functional difficulties and the pathways that drive the deprivations and inequalities that are highlighted. This should be the subject of further research.
Nonetheless, results from this Report contribute to a growing international literature on disability and gender inequalities by providing estimates for women in 35 countries right before the COVID-19 pandemic broke out.
TABLE 4.1: Indicators under study
| Indicator | CRPD Article | SDG indicator | Results table |
|---|---|---|---|
| Education | |||
| Women who have ever attended school | 24 | E1 | |
| Women who have less than primary school completion | 24 | E2 | |
| Women who have completed primary school | 24 | E3 | |
| Women who have completed secondary school or higher | 24 | E4 | |
| Literacy rate | 24 | 4.6.1 | E5 |
| Personal activities | |||
| Women who, at least once a week, read a newspaper or magazine, listen to the radio, and watch television |
9 | P1 | |
| Women who used a computer during the last 3 months | 9 | P2 | |
| Women who used the internet during the last 3 months | 9 | P3 | |
| Women who own a mobile phone | 9 | 5.b.1 | P4 |
| Health | |||
| Women in households using safely managed drinking water | 25 | 6.1.1 | H1 |
| Women in households using safely managed sanitation services | 25 | 6.2.1 | H2 |
| Women with family planning needs met | 6, 25 | 3.7.1/5.6.1 | H3 |
| Women reporting they did not participate in activities due to menstruation | 25 | H5 | |
| Women who think husband is justified to hit wife | 16, 25 | 16.1.3 | H6 |
| Women reporting having heard of HIV | 25 | H7 | |
| Women who correctly identified all three means of mother-to-child transmission of HIV | 25 | H8 | |
| Women who have ever been tested for HIV | 25 | H9 | |
| Standard of living | |||
| Women in households with electricity | 28 | 7.1.1 | S1 |
| Women in households with clean cooking fuel | 28 | 7.1.2 | S2 |
| Women in households with adequate housing | 28 | S3 | |
| Women in households owning assets | 28 | S4 | |
| Women in households with a mobile phone | 28 | 5.b.1 | S5 |
| Multidimensional poverty | |||
| Women who experience multidimensional poverty, i.e. deprivations in more than one dimension of wellbeing (education, health, standard of living) |
24, 25, 28 | M1 | |
| Insecurity | |||
| Women covered by health insurance | 28 | 1.3.1/3.8.1 | I1 |
| Women in households receiving social protection | 28 | 1.3.1 | I2 |
| Women years feeling safe walking alone in their neighborhood after dark | 16 | 16.1.4 | |
| Women having personally felt discriminated against or harassed on the basis of disability |
5 | 10.3.1 /16.b.1 | I3 |
| Women having personally felt discriminated against or harassed on the basis of a gender | 5 | 10.3.1 /16.b.1 | I4 |
| Women having personally felt discriminated against or harassed on the basis of any ground of discrimination prohibited under international human rights law |
5 | 10.3.1 /16.b.1 | I5 |
| Subjective wellbeing | |||
| Women who are very or somewhat happy | SW1 | ||
| Women whose life improved during the last one year and who expect that their life will be better after one year |
SW2 | ||
| Mean life satisfaction ladder for women: women were asked to consider where they situate their life on a ladder with steps numbered from 0 at the bottom (worst possible life) to 10 at the top (best possible life). |
SW3 | ||
Notes: Indicators are described in Appendix 3 Method Brief #2. Indicator H4 is not available in this Report (it was available in the 2021 Report). Literacy is captured through the ability to read a short simple statement about everyday life or who attended secondary or higher education. Attitude toward domestic violence is the share of women who state that a husband is justified in hitting or beating his wife in relation to housework in at least one of the following circumstances: (1) she goes out without telling him, (2) she neglects the children, (3) she argues with him, (4) she refuses sex with him, and/or (5) she burns the food.
Figure 4.2: Among those with any functional difficulties, share with difficulty by domain (%)
[5] In fact, the answer scale for the sixth question of the WGSS on difficulty communicating does not have level 4 (cannot do at all).
[6] Here are the countries where we found the Adult Functioning questionnaire for men: Belarus, Central African Republic, Chad, Cuba, Democratic Republic of Congo, Georgia, Ghana, Guinea Bissau, Gambia, Guyana, Honduras, Iraq, Kiribati, Kosovo, Lesotho, Madagascar, Malawi, Mongolia, Montenegro, Nepal, Sao Tome, Sierra Leone, Suriname, Togo, Tonga, Tunisia, Zimbabwe.
[7] Population statistics were not available for Kosovo, which is therefore not included in cross country estimates.
[8] In some countries, a randomly chosen male respondent aged 18 to 49 also answered.
[9] The 30 to 44 age bracket is consistent with the age categories analyzed in the 2021 Report and was maintained for comparability.